Heart rate variability (HRV) stands as one of the most reliable measures for assessing autonomic nervous system (ANS) function. This reliability is particularly evident when controlled maneuvers such as the Valsalva maneuver, deep breathing (DB), and head-up tilt challenge are employed, as outlined by [6]. The high reproducibility of ANS function testing, coupled with the relatively straightforward nature of these tests, makes them invaluable tools.
The evaluation of autonomic function serves a dual purpose: it can either confirm the normal operation of the ANS or play a crucial role in studies concerning autonomic dysfunction or neuropathy. The ANS operates through a dynamic interplay between its two branches: the parasympathetic nervous system (PNS) and the sympathetic nervous system (SNS). Any shifts in the balance between sympathetic and parasympathetic activations are readily reflected in the results of ANS tests, as elaborated upon herein.
Changes to ANS function can manifest as either temporary or permanent alterations. Temporary changes may result from factors such as increased sympatho-vagal balance due to sporadic psychosocial or physiological stressors, or during infections. On the other hand, permanent autonomic dysfunction typically stems from chronic diseases, like diabetes, leading to autonomic neuropathy. Moreover, the process of aging itself has been associated with diminished ANS functioning.
Standard tests for assessing autonomic nervous system function include the Valsalva maneuver, deep breathing (DB), and head-up tilt challenge, collectively referred to as the Ewing tests, as introduced by [2]. In the following sections, we will delve into these tests and the associated data analytics.
Valsalva maneuver
During the Valsalva maneuver, the subject forcefully exhales into a mouthpiece, generating a pressure of 40 mmHg for a duration of 15 seconds. This maneuver allows us to assess autonomic nervous system function and observe the heart rate response during and after its execution.
- During the maneuver, heart rate typically increases owing to heightened sympathetic activity. This sympathetic response is triggered by a reduction in aortic blood pressure caused by increased intrathoracic pressure, diverting blood away from the heart.
- Immediately after the maneuver, heart rate continues to increase briefly. This elevation is a consequence of both the natural reflex to take a deep breath after the maneuver, leading to vagal inhibition, and the somewhat delayed response of the sympathetic nervous system.
- Shortly after the maneuver, heart rate decreases due to a sudden rise in blood pressure, which activates baroreceptors and initiates parasympathetic cardiac activity. The elevation in blood pressure is a result of blood returning to the heart, as intrathoracic pressure returns to normal, and partly due to lingering sympathetic activity causing peripheral vasoconstriction.
Valsalva ratio
The Valsalva ratio is calculated as the ratio of the longest RR interval shortly (0-30 seconds) after the maneuver to the shortest RR interval during or immediately (0-5 seconds) after the maneuver. To enhance the accuracy of the Valsalva ratio, it is computed using 5-beat average values for both the longest and shortest intervals. A typical heart rate response to the Valsalva maneuver is illustrated in Figure 1.
For healthy adults, a Valsalva ratio value of 1.2 or higher is considered normal, as indicated by [1], [2], [4], [5], [6], and [9]. Ewing et al. (1985) also classify a value between 1.1 and 1.2 as a borderline case, and a value of 1.1 or lower as abnormal. Additionally, Risk et al. (2001) provide normative values for the Valsalva ratio, taking age and gender into account. For healthy women aged 20-80 years, the average ratio linearly decreases with age, ranging from about 2.1 to 1.4, while the same age-dependent decrease for men ranges from 2.1 to 1.3. Age-related lower normal limits for the Valsalva ratio are summarized in Table 1.
In Kubios HRV software, the Valsalva ratio value is represented using a four-zone model based on the normal values reported for healthy adults: VERY LOW (1.00–1.10), LOW (1.10–1.20), NORMAL (1.20–2.10), and HIGH (2.10–3.00). A Valsalva ratio falling into the VERY LOW zone is considered abnormally low for healthy adults of all ages. Younger adults (under 40 years) are expected to have Valsalva ratios in the NORMAL or HIGH zones.


Figure 1: Heart rate response to Valsalva maneuver in a healthy individual, including RR interval data, 5-beat averaged data, and the Valsalva ratio (RR max / RR min).
Deep breathing test
During the deep breathing challenge, participants are instructed to inhale and exhale at a rate of six breaths per minute, corresponding to a respiratory rate of 0.10 Hz. This controlled breathing should be paced either by a metronome or a similar device, or alternatively, by using a prepared deep breathing pacing video. The following section provides an overview of autonomic nervous system function and the heart rate response elicited during the deep breathing challenge.
- During inhalation, the diaphragm contracts, moving downward to expand the chest cavity, and simultaneously reducing intrathoracic pressure to facilitate air intake into the lungs. This decrease in arterial blood pressure deactivates baroreceptors and diminishes vagal tone, resulting in an increase in heart rate.
- During exhalation, the diaphragm relaxes, moving upward, compressing the chest cavity, and raising intrathoracic pressure, which expels air from the lungs. This increase in arterial blood pressure activates baroreceptors and leads to a reduction in heart rate.
As a consequence, the heart rate of a healthy individual exhibits distinct modulations in response to the breathing frequency—accelerating during inhalation and decelerating during exhalation. These fluctuations in heart rate can be easily observed even by manually checking the pulse from the wrist while engaging in deep breathing exercises.
HR response to deep breathing
To assess the heart rate response to deep breathing, we detect the longest RR interval observed at the end of the expiration phase and the shortest RR interval observed at the end of the inspiration phase. These intervals are then averaged over the respiratory cycles occurring during the challenge. The heart rate (HR) response is quantified as the difference between the maximum and minimum heart rates in beats per minute, computed from the averaged RR interval extrema points. Alternatively, the response to deep breathing may be reported as the difference (E-I) or the ratio (E/I) between the averaged RR interval extrema points:

Here, RRmax represents the average of the longest RR intervals observed at the end of the exhale phase, and RRmin represents the average of the shortest RR intervals observed at the end of the inhale phase. A typical heart rate response to the deep breathing challenge is illustrated in Figure 2.
For healthy adults, a HR response of 15 bpm or higher is considered normal, 10-15 bpm is borderline, and lower than 10 bpm is abnormal, as per [2], [3}, and [9]. Similarly, the E/I ratio in young adults should be higher than 1.2 (Zygmunt & Stanczyk, 2010). Both HR response and the E/I ratio are influenced by age. In healthy adults aged 16-70 years, the average E/I ratio decreases from 1.62 to 1.20 [7]. It’s worth noting that the E/I ratio is also significantly affected by the resting heart rate, as lower resting HR values lead to higher E/I ratios, even if the HR response (i.e., the difference between the maximum and minimum heart rates) remains constant. Age-related lower normal limits for the deep breathing challenge are summarized in Table 1.
In Kubios HRV software, the HR response to deep breathing is represented using a four-zone model based on normal values reported for healthy adults: VERY LOW (0–6 bpm), LOW (6–11 bpm), NORMAL (11–35 bpm), and HIGH (35–55 bpm). An HR response falling into the VERY LOW zone is considered abnormally low for healthy adults of all ages. Younger adults (under 40 years) are expected to have an HR response in the NORMAL or HIGH zones.
HRV during the deep breathing test
The resting heart rate, or mean HR during deep breathing, should typically be below 100 bpm. Additionally, we can calculate the magnitude of respiratory sinus arrhythmia (RSA) as the spectral amplitude of RR interval fluctuations centered at the breathing frequency. RSA magnitude describes the extent of HRV associated with breathing. Secondly, the PNS index provides an indication of the subject’s resting HRV compared to normal values in the adult population. Finally, other commonly used HRV measures, such as RMSSD or SDNN, may also be employed to characterize HRV magnitude during the deep breathing challenge.

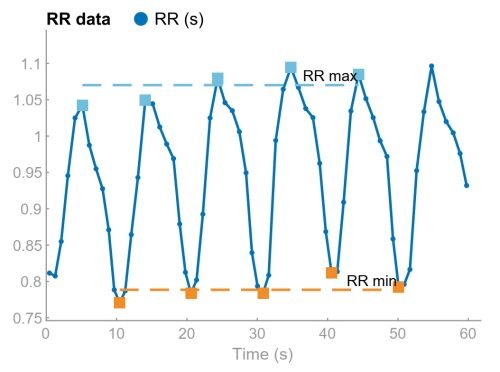
Figure 2: Heart rate response to deep breathing challenge in a healthy individual, including RR interval data, RR interval extrema points, and the HR response (HR max-HR min).
Head-up tilt test
The third standard autonomic function test involves evaluating the heart rate response to a head-up tilt. This test is typically conducted by instructing the subject to stand up after resting in a supine position (“active tilt”) or by tilting the subject from a supine to an upright position using a tilt table (“passive tilt”). To ensure accurate assessment of HR response and heart rate variability (HRV), both the supine and upright positions should be maintained for at least 5 minutes. Let’s delve into what transpires within the autonomic nervous system during this test.
- In the supine position, our body is at rest, and the parasympathetic tone of the autonomic nervous system is dominant. Consequently, our heart rate is low, and heart rate variability is high during supine rest.
- The head-up tilt induces a significant shift in blood from the upper body to the abdomen and lower extremities, reducing blood volume in the upper body. This results in a decrease in cardiac output and blood pressure. To counteract this abrupt drop in blood pressure, the sympathetic nervous system is activated, leading to an increase in heart rate and peripheral vasoconstriction.
- Following the tilt, heart rate gradually increases and peaks around 15 seconds after the change in posture. Soon after, a new baseline is established as the balance between sympathetic and parasympathetic activities stabilizes. In the upright position, the mean heart rate is higher, and HRV is lower, especially the indexes sensitive to parasympathetic nervous activity, when compared to the supine position.
30:15 ratio
Ewing et al. (1985) observed that heart rate reaches its maximum around the 15th beat after assuming an upright position, followed by relative bradycardia, causing the heart rate to reach a local minimum around the 30th beat. The ratio between the longest RR interval around the 30th beat and the shortest RR interval around the 15th beat is defined as the 30:15 ratio.
For healthy adults aged 16-69 years, the average 30:15 ratio was 1.29, with a value of 1.05 or higher considered normal [1], [2], [9]. Age-related lower normal limits for the 30:15 ratio are summarized in Table 1.
In Kubios HRV software, the 30:15 ratio is represented using a four-zone model based on normal values reported for healthy adults: VERY LOW (1.00–1.02), LOW (1.02–1.05), NORMAL (1.05–1.35), and HIGH (1.35–1.80). A 30:15 ratio falling into the VERY LOW zone is considered abnormally low for healthy adults of all ages. Younger adults (under 40 years) are expected to have a 30:15 ratio in the NORMAL or HIGH zones.
HRV measures of head-up tilt test
Various HRV parameters can be assessed to examine how autonomic function changes during the transition from a supine to an upright position. The supine position provides resting heart rate and resting HRV values during spontaneous breathing. The PNS index should decrease as it indicates the decrease in HRV associated with parasympathetic nervous activity due to the postural change. Standard time-domain and frequency-domain HRV parameters can further elucidate the change in ANS function. Specifically, the low-frequency (LF) and high-frequency (HF) spectral components of HRV are valuable in assessing the shift in sympatho-vagal balance. However, it’s crucial to ensure that the respiratory rate is within the HF band, and the software’s validated respiratory rate (RESP) estimate is useful in this regard.


Figure 3: Heart rate response to head-up tilt challenge in a healthy individual, including RR interval data, 5-beat averaged data, and the 30:15 ratio (RR30 / RR15).
Table 1: Age related lower limits for Valsalva maneuver, deep breathing and head-up tilt test results
| Age (years) | 20 | 25 | 30 | 35 | 40 | 45 | 50 | 55 | 60 | 65 |
|---|---|---|---|---|---|---|---|---|---|---|
| Valsalva maneuver | ||||||||||
| Valsalva ratio | 1.22 | 1.22 | 1.21 | 1.20 | 1.19 | 1.19 | 1.18 | 1.17 | 1.17 | 1.16 |
| Deep Breathing | ||||||||||
| HR response | 13 | 12 | 11 | 11 | 10 | 9 | 9 | 8 | 8 | 7 |
| E-I (ms) | 136 | 127 | 119 | 112 | 105 | 98 | 92 | 86 | 81 | 76 |
| E/I | 1.20 | 1.18 | 1.16 | 1.14 | 1.13 | 1.12 | 1.11 | 1.10 | 1.09 | 1.08 |
| RMSSD (ms) | 19 | 18 | 16 | 15 | 14 | 13 | 12 | 11 | 10 | 9 |
| Head-up tilt | ||||||||||
| 30:15 ratio | 1.15 | 1.14 | 1.12 | 1.11 | 1.10 | 1.09 | 1.08 | 1.07 | 1.07 | 1.05 |
| RMSSD (supine) | 16 | 15 | 13 | 11 | 10 | 9 | 8 | 7 | 6 | 6 |
Values are derived from Smith 1982, Ziegler et al. 1992, and Baron & Ewing 1999.
Frequently asked question (FAQ)
What is autonomic nervous system function analysis?
Autonomic nervous system function analysis involves assessing how the autonomic nervous system (ANS) regulates body processes like heart rate, blood pressure, and breathing. This analysis helps understand the balance between the sympathetic and parasympathetic branches of the ANS, providing insights into stress response, relaxation states, and overall health.
What are the Ewing’s battery tests?
The Ewing’s battery is a series of tests used to assess the autonomic nervous system’s function, particularly in people with diabetes or suspected autonomic dysfunction. These tests measure responses to various stimuli, such as the Valsalva maneuver, deep breathing, and lying to standing, to detect abnormalities in cardiovascular autonomic control.
How does Kubios software analyze autonomic nervous system function?
Kubios software calculates the standard ANS function parameters such as the Valsalva ratio, HR response to deep breathing, and the 30:15 ratio for head-up tilt. In addition, Kubios HRV software analyzes autonomic nervous system function by using heart rate variability (HRV) metrics to provide a detailed view of the sympathetic and parasympathetic nervous system activities.
How to detect autonomic nervous system dysfunction?
Autonomic nervous system dysfunction can be detected through abnormal heart rate and heart rate variability responses, fluctuations in blood pressure, and other clinical symptoms. Ewing’s battery tests and other clinical assessments are used to evaluate the extent and nature of the dysfunction in the ANS.
References
- Baron R and Ewing DJ. Heart rate variability. In Recommendations for the Practice of Clinical Neurophysiology: Guidelines of the International Federation of Clinical Physiology (Eds. Deuschl G and Eisen A), Chapter 7.2, pp. 283-286, 1999.
- Ewing DJ, Martyn CN, Young RJ, and Clarke BF. The value of cardiovascular autonomic function tests: 10 years experience in diabetes. Diabetes Care, 8:491-498, 1985.
- Hilz MJ and Dütsch M. Quantitative studies of autonomic function. Muscle Nerve. 33(1):6-20, 2006.
- Jha RK, Acharya A, and Nepal O. Autonomic influence on heart rate for deep breathing and valsalva maneuver in healthy subjects. J Nepal Med Assoc, 56(211):670-673, 2018.
- Novak P. Quantitative autonomic testing. J Vis Exp, 53(e2502):1-24, 2011.
- Risk M, Bril V, Broadbridge C, and Cohen A. Heart rate variability measurement in diabetic neuropathy: review of methods. DiabetesTechnol & Therap, 3(1):63-76, 2001.
- Smith SA. Reduced sinus arrhythmia in diabetic autonomic neuropathy: diagnostic value of an age-related normal range. Br Med J, 285:1599-1601, 1982.
- Ziegler D, Laux G, Spüler M, Mühlen H, Mayer P, and Gries FA. Assessment of cardiovascular autonomic function: age-related normal ranges and reproducibility of spectral analysis, vector analysis, and standard tests of heart rate variation and blood pressure responses. Diabetic Med, 9(2):166-175, 1992.
- Zygmunt A and Stanczyk J. Methods of evaluation of autonomic nervous system function. Arch Med Sci, 6(1):11-18, 2010.